Laparoscopic Pyeloplasty
Laparoscopic pyeloplasty is a minimally invasive method for performing reconstructive surgery on a constriction or scarring in the ureter (the tube that empties urine from the kidney to the bladder).
This procedure is intended to treat a blockage or narrowing of the ureter as it exits the kidney. This anomaly is known as ureteropelvic junction (UPJ) blockage, which causes poor and slow urine outflow from the kidney. UPJ blockage may result in stomach and flank discomfort, stones, infection, elevated blood pressure, and impairment of kidney function.
When compared to the traditional open surgical approach, laparoscopic pyeloplasty has resulted in much less post-operative discomfort, a shorter hospital stay, a faster return to work and daily activities, a more attractive esthetic result, and results that are comparable to the open operation.
The Surgery
Obstruction at the ureteropelvic junction (UPJ)
Laparoscopic pyeloplasty is done under general anesthesia. The surgery typically takes three to four hours. The procedure is conducted via three tiny (1 cm) abdominal incisions. A telescope and tiny equipment are sent into the belly via these keyhole incisions, allowing the surgeon to fix the blockage/narrowing without having to enter his or her hands.
At the completion of the treatment, a tiny plastic tube (known as a ureteral stent) is left within the ureter to bridge the pyeloplasty repair and assist with kidney drainage. This stent will stay in place for four weeks before being removed at the doctor’s office. A tiny drain will also be placed in your flank to remove any fluid surrounding the kidney during the pyeloplasty procedure.
Potential Risks and Complications
Diagram for kidney surgery
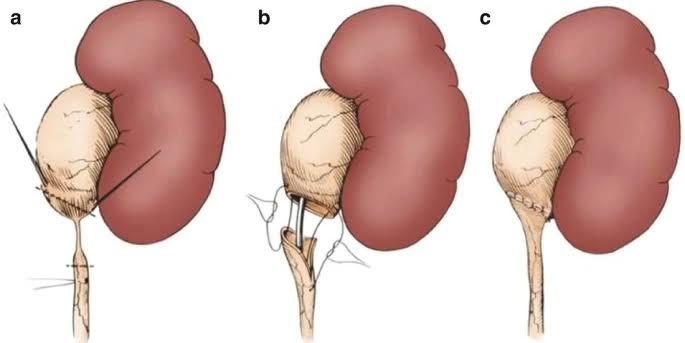
Laparoscopic dismembered pyeloplasty.
Although this operation has been shown to be quite safe, there are risks and possible problems, just like any other surgery. In comparison to open surgery, the safety and complication rates are comparable. Potential dangers include:
Bleeding: During this treatment, blood loss is usually minimal (less than 100 cc), and a blood transfusion is seldom necessary. If you are still interested in autologous blood transfusion (donating your own blood) before your operation, you must notify your surgeon. When the information package for your procedure is sent or delivered to you, you will be given a permission form to send to your local Red Cross.
Infection: All patients are given broad-spectrum intravenous antibiotics before surgery to reduce the possibility of infection thereafter. If you have any indications or symptoms of infection after surgery (fever, discharge from your incision, urine frequency, discomfort, pain, or anything else you are worried about), please call us right away.
Hernias at incision sites are uncommon since all keyhole incisions are meticulously closed at the end of your procedure.
Tissue/organ injury: Although rare, injuries to surrounding tissue and organs such as the colon, vascular structures, spleen, liver, pancreas, and gallbladder may need further surgery. Positioning-related neurons or muscles may be injured.
Conversion to open surgery: If the laparoscopic technique proves to be too challenging, it may be necessary to convert to open surgery. This might result in a bigger conventional open incision and a lengthier recovery time.
Failure to repair UPJ obstruction: About 3% of patients who have this procedure will have chronic blockage because of repeated scarring. If this happens, further surgery may be required.