Megaureters
Megaureters: what are they?
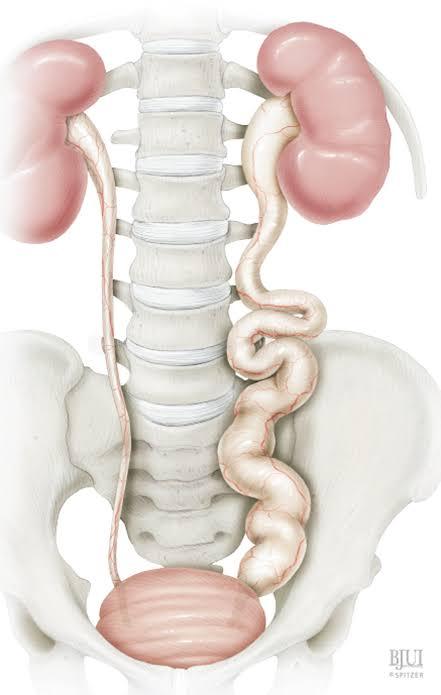
The word “megaureter,” which translates to “big ureter,” is descriptive rather than diagnostic. Whether the megaureter is caused by backwash, or urine reflux, or by obstruction at the ureterovesical junction, are the two key concerns regarding megaureters. The diagnosis of “refluxing megaureter” or “megaureter from reflux” is made if reflux occurs. “Obstructed megaureter” or “primary obstructed megaureter” are the diagnoses if blockage is present. “Primary non-obstructed megaureter” is the diagnosis if neither reflux nor blockage is present. Rarely, reflux and blockage may occur; in these cases, the condition is known as “refluxing obstructed megaureter.” The “primary non-obstructed megaureter” and the “refluxing megaureter” are by far the two most popular kinds of megaureters.
What signs of a megaureter are present?
Megaureters are often seen on prenatal ultrasounds and are asymptomatic. However, a child’s urinary tract infection may also lead to the discovery of megaureters. Additionally, there may infrequently be blood in the urine or flank discomfort.
How do you detect a megaureter?
The phrase “megaureter” simply refers to a huge ureter, which is identified by ultrasonography. Following the discovery of a megaureter, two more tests are often carried out to check for blockage or reflux. To check for reflux, a VCUG is done. To check for obstructions and assess how effectively the kidneys work in relation to one another, a lasix renal scan is conducted.
What is the treatment for megaureters?
The origin of megaureters determines how they are treated. Prophylactic antibiotics and, if necessary, endoscopic or open surgery are used to address reflux that is producing the megaureter. A number of criteria are taken into account when suggesting therapy if there is blockage or partial obstruction causing the megaureter at the ureterovesical junction. A ureteral reimplant (see section on ureteral reimplantation) with blockage removal is advised if the kidney with the partly or completely blocked megaureter has diminished function or if recurrent UTIs occur. However, surgery may often be avoided if the kidney is working normally and the blocked or partly obstructed megaureter is not producing symptoms. This is because the blockage may eventually clear itself and the megaureter may disappear.
Most of these measures go away with time if there is no blockage or reflux, and only sporadic ultrasounds are used to evaluate kidney development.
The majority of megaureter patients will be prescribed preventative antibiotics until the megaureter disappears on its own, toilet training is finished, or, in the event that surgery is necessary, once the procedure is finished.
Megaureters are treated for what reason?
Megaureters are treated to avoid kidney damage and urinary tract infections, regardless of whether they are caused by reflux or blockage. Kidney injury may result from blockage or reflux, particularly when urinary tract infections are present. Because urinary tract infections are more likely to occur, prophylactic antibiotics may be used. Additionally, surgery could be necessary.
After therapy, what happens?
For megaureters brought on by reflux, please refer to the section on vesicoureteral reflux.
Prophylactic antibiotics are often used for a while after surgery for megaureters that need it, and the kidney is monitored with repeated ultrasounds. The impediment is successfully removed by the procedure.
Megaureters that do not have blockage or reflux usually go away on their own in childhood. In order to track kidney development and the megaureter, prophylactic antibiotics are often administered until toilet training is complete. After the megaureter resolves, preventive antibiotics and further monitoring are not required.
The great majority of kids with megaureters go on to lead normal lives, even if surgery is required.