Posterior Urethral Valves
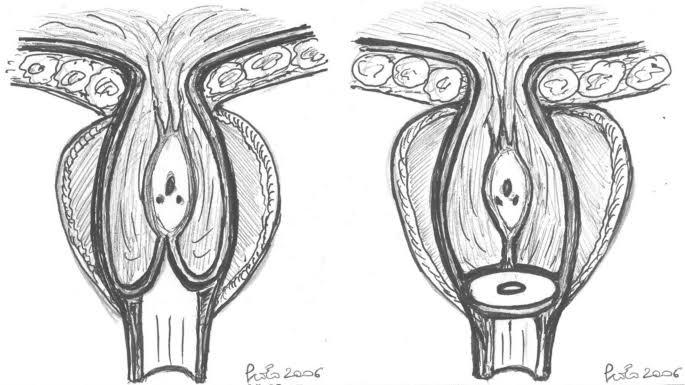
What Are They? Urine is transported from the bladder to the outside of the body by the urethra, a tube. In a condition known as posterior urethral valves (PUV), extra tissue flaps develop inside the urethra and partially obstruct urine flow, analogous to how spinnakers on a sailboat obstruct wind flow. PUV is a congenital condition, meaning that it is present from birth. It may have an impact on the unborn child while it is still in the womb. (foetus).
Why does PUV occur? Boys are nearly the only ones with posterior urethral valves. Between 1 in 5,000 and 1 in 8,000 male babies are affected by PUV. PUV is not a hereditary disorder. To put it another way, PUV cases are random and do not transmit from one generation to the next. It is extremely uncommon for PUV to impact multiple family members.
How is PUV diagnosed? The physician will perform a physical examination and a thorough medical history. Additionally, a few medical tests will be ordered, including:
• A voiding cystourethrogram, a unique x-ray of the bladder and urethra that can reveal urethral blockage. Additionally, this test determines whether the patient has vesicoureteral reflux, which affects roughly 30 to 50 out of every 100 PUV patients.
• Ultrasound: A kidney ultrasound provides us with an estimate of the amount of kidney tissue and displays the dilatation of the kidney and ureter.
• Certain blood tests evaluate kidney function.
Prenatal, or antenatal, diagnosis
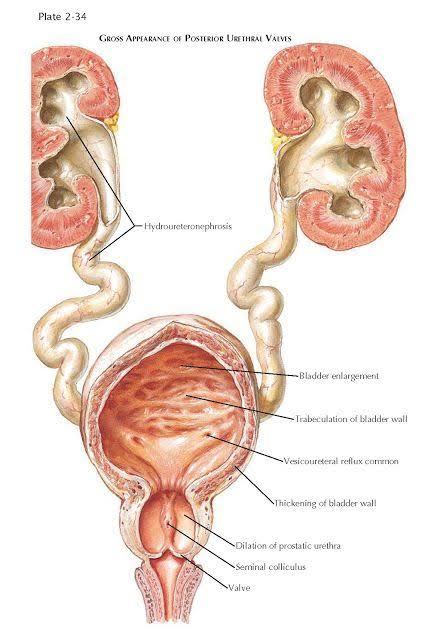
More PUV patients are diagnosed in the uterus before birth as a result of the increased use of ultrasound during pregnancy. An antenatal ultrasound displays pictures of the amniotic sac and the unborn child. It may also exhibit issues like oligohydramnios, which is the compression of the foetus in the uterus, and/or dilated kidneys and ureters that could be brought on by PUV. What issues are brought on by PUV? The most frequent cause of severe forms of paediatric urinary tract obstructions (blockages) is PUV. It causes a number of issues.
• Bladder hypertrophy: The extra effort required to void can cause the muscles of the bladder wall to thicken and enlarge, much like a body builder’s muscles do with exercise. In contrast to bodybuilders, the bladder may swell and stretch until the muscles are overextended and unable to function. Intermittent catheterisation may be necessary for this condition in order to empty the bladder.
• Vesicoureteral reflux: Urine may flow backwards from the bladder to the kidney as a result of the valves. As a result, the kidney and ureters—the tube that joins the bladder and kidney—widen (dilate). This significantly raises the risk of kidney damage and infections.
• Renal dysplasia: this condition is characterised by aberrant kidney development linked to posterior urethral valves. Poor or nonexistent kidney function is a result of dysplastic kidneys. Severe posterior urethral valve disease in the foetus can cause potentially fatal issues:
• If urine flow is impeded or blocked, kidney failure and body salt (sodium) imbalances may result.
• Oligohydramnios: if the foetus produces too little urine, it may compress inside the uterus. Foetal compression may result from this because there is less fluid in the amniotic sac, which is made up of foetal urine. Oligohydramnios can result in underdeveloped lungs, growth restriction, and bony abnormalities of the face and limbs. Vesicoureteral reflux, partial renal failure, and improper bladder voiding are some of these chronic issues.
How are PUV patients treated? A tiny catheter is inserted into the infant’s bladder to remove the urine in order to relieve a severe obstruction. With an IV, infants can also get additional fluid and sodium straight into their bloodstream. Until the infant can breathe on his own, mechanical ventilation is used if lung function is compromised. The infant is given antibiotics if there is an infection.
Laser PUV fulguration: Valve ablation is the surgical procedure used to remove the posterior urethral valves. Since this is an endoscopic procedure, no surgical incision is necessary. A cystoscope, which is a tiny tube with a light and a camera lens at the end, is inserted straight into the urethra by the physician. Then, using a holmium laser fibre that has been inserted through the cystoscope, the doctor makes incisions in the valves to cause them to collapse and no longer block the urethra.
Other surgical options are required to divert the flow above the level of the urethra if valve ablation does not improve kidney function, which can occasionally happen in severe cases. There are a number of choices for this: • A vesicostomy is the direct opening of a tiny section of the bladder to the skin. A ureterostomy is when a section of the ureter is opened straight to the skin. During a pyelostomy, the kidney’s urine is extracted straight from the skin that covers it. By optimising the flow of urine from the kidneys, these procedures reduce infections and enhance kidney function. The disadvantage is that additional surgery will be required in the future to restore the flow of urine to the bladder.
Additional surgeries could result from PUV complications. 1. Surgery to increase the bladder’s safe capacity to hold urine is known as bladder augmentation. 2. If PUV results in renal failure, a kidney transplant may be required. A safe urinary reservoir for a future kidney transplant could be made possible by bladder augmentation.