Kidney Stone Treatment
Kidney stones are what?
The kidney develops kidney stones. A stone is referred to as a ureteral stone if it exits the kidney and becomes lodged in the ureter. Numerous salts and minerals are dissolved in urine. When urine contains high concentrations of certain minerals and salts, stones may develop. Small kidney stones may not initially cause any problems. Kidney stones, however, have the potential to enlarge and potentially fill the kidney’s internal hollow structures. Some kidney stones remain there and never cause any issues.
Sometimes kidney stones can move down the ureter. (The tube that connects the kidney and bladder is called the ureter.) The stone may be expelled from the body through urine if it makes it to your bladder. Urine flow from that kidney is blocked if the stone lodges in the ureter. This might hurt.
What are the signs of Kidney Stones?
· Sharp, cramping pain in the side and back is a common sign of kidney stones. This sensation frequently spreads to the groin or lower abdomen. Often, the pain begins abruptly and develops gradually. As the body works to remove the stone, it may come and go.Additional indicators of kidney stones include:
· The sensation of having to urinate.
· frequent urination or a burning sensation during urination.
· blood-colored urine that is dark or red. (Occasionally, urine contains very minute numbers of red blood cells that are invisible to the unaided eye.)
· vomiting and nausea.
· Men get pain near the tip of their penis.
What Constitutes Kidney Stones?
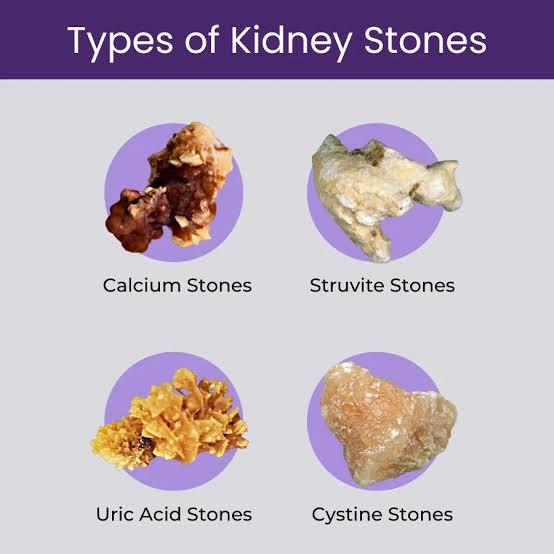
There are numerous varieties and hues of kidney stones. The sort of kidney stone you have will determine how it is treated. Your stone kind will also determine how to stop new stones from developing.
· Calcium Stones – Eighty percent of stones are calcium stones. The most prevalent kind of stones are calcium stones. Calcium phosphate and calcium oxalate are the two forms of calcium stones. More prevalent is calcium oxalate. The risk is increased for those whose urine contains excessive amounts of calcium. Calcium stones can develop for different reasons even when there is a normal level of calcium in the urine.
· Uric Acid stones – Five to ten percent of stones are uric acid stones, which are waste products from bodily chemical reactions. Urine that is acidic does not dissolve uric acid crystals well. Rather, a uric acid stone will form. Urine that is acidic can result from:
o Being overweight
o Prolonged diarrhoea
o Diabetes type 2 (high blood sugar)
o Gout
o A diet that is low in fruits and vegetables and high in animal protein
· Struvite – 10% of stones are struvite or infection stones, which are an uncommon kind of stone. Chronic urinary tract infections are linked to these stones. The most vulnerable to these stones are those who suffer from persistent urinary tract infections or who have neurological conditions that impair their ability to empty their bladder.
· Cystine – Less than 1% of stones are cysteine-containing, which is an amino acid found in some meals. It is among the components that make up proteins. An uncommon, hereditary metabolic disease is cystinuria, or having too much cystine in the urine. It occurs when cystine in the urine is not reabsorbed by the kidneys. Stones occur when the urine contains high levels of cystine. Childhood is often when cystine stones first appear.
Diagnosis of Kidney Stones
· Imaging – USG , CT scan, Xray KUB
· Urine – Urine routine examination and culture
· 24 hr urine analysis for recurrent stone formers
· Renal function tests
· Stone analysis if stones are removed or passed out
Kidney stone treatment
Kidney stone treatment is dependent on the following:
· The kind of stone you possess
· The stone’s location
· How severe it is and how long have you been experiencing symptoms?
A. Wait and watch – A stone will usually pass by itself if you just wait for it to do so. Compared to larger stones, smaller stones are more likely to pass by themselves. The stones are eliminated when the body passes urine normally. As long as the kidney is not completely blocked, the discomfort is tolerable, there are no indications of infection, and the stone is small enough to clear, waiting up to six weeks for it to pass is safe. Drink as much water as usual as you wait for the stone to pass. When the pain is severe, you might need to take medicine.
B. Medication: It has been demonstrated that several drugs can aid in the passage of stones. Tamsulosin is the most often prescribed medication. By relaxing the ureter, tamsulosin facilitates the stone’s passage. While you wait, you could also require pain and nausea medication.
C. Surgery: If a kidney or ureter stone does not pass, surgery may be required to remove it. Indications of removal
a. It is too painful to wait for the stone to go away.
b. Kidney function is being impacted by the stone.
The following procedures are used to remove kidney or ureter stones:
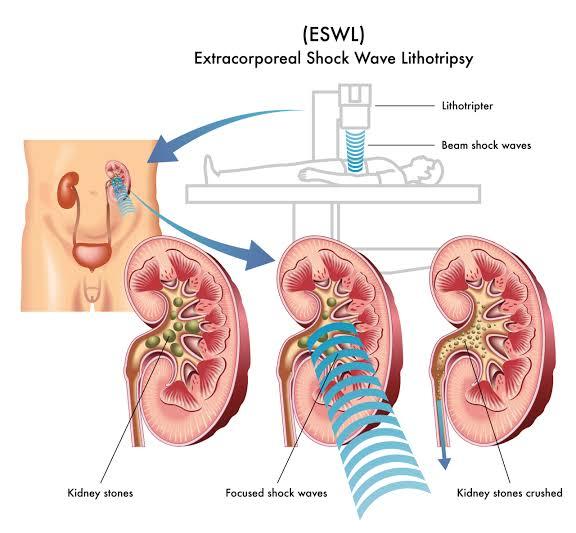
i. ESWL – The procedure known as Shock Wave Lithotripsy (SWL) is used to treat kidney and ureter stones. To locate the stone, X-rays or ultrasound are utilised to focus shock waves on it. The stone typically breaks into tiny fragments when shock waves are fired at it repeatedly. Over a few weeks, these tiny stone fragments dissolve in the urine. Ask your doctor what the best course of action is for your stone because not all stones respond well to SWL.
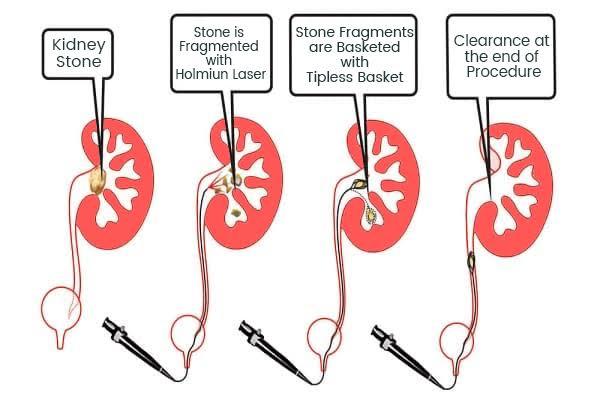
ii. URS (URSL/RIRS) – The procedure known as ureteroscopy (URS) is used to treat kidney and ureteric stones. A tiny telescope known as a ureteroscope is sent into the bladder, up the ureter, and into the kidney during URS. For stones in the lower portion of the ureter close to the bladder, rigid telescopes are utilised. Kidney and upper ureter stones are treated with flexible telescopes. The urologist can view the stone using the ureteroscope without cutting. You remain calm throughout the URS process thanks to general anaesthesia. Smaller stones are caught and removed by a tiny, basket-like device once the urologist has seen the stone with the ureteroscope. A laser or other stone-breaking equipment can be used to shatter huge stones into smaller pieces if they cannot be removed in one piece. Your doctor might insert a temporary stent in the ureter once the stone has been extracted, either completely or in fragments. A small, stiff plastic tube called a stent aids in keeping the ureter open, allowing urine to flow from the kidney into the bladder. This tube is internal to the body and does not require a bag to collect urine, in contrast to a kidney drainage tube or bladder catheter. In two to three days, you can resume your regular activities after returning home on the same day as the URS. Your urologist will remove the stent four to ten days after it is placed. To enable self-removal, a string is occasionally left on the end of the stent. Taking your doctor’s advise regarding when to remove the stent is very important. Long-term usage of the stent may result in infection and renal impairment.
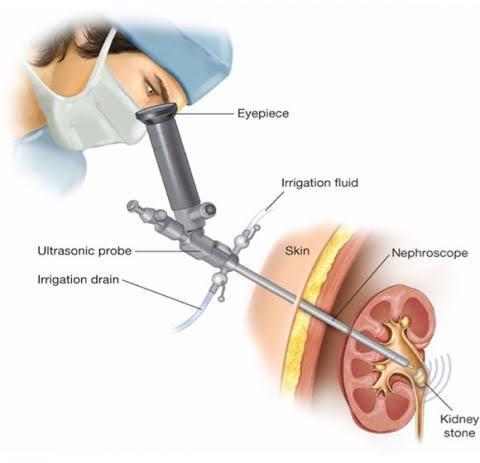
iii. Percutaneous Nephrolithotomy (PCNL): The most effective treatment for kidney stones that are big is PCNL. To perform a PCNL, general anaesthesia is required. PCNL entails creating a half-inch incision (cut) in the side or back of the kidney that is just big enough to fit a rigid telescope (nephroscope) into the kidney’s hollow centre, where the stone is placed. The stone is broken apart and the fragments are sucked out by a tool that is passed through the nephroscope. PCNL is the greatest option for treating big stones because it can suction fragments. Urine may be drained into an external bag via a tube that is left in the kidney following the PCNL. This will prevent any bleeding and let urine to drain. The tube is left in for a few days or overnight. Following this surgery, you might need to spend the night in the hospital. In order to control recovery, a temporary stent could also be left in place. While you are still in the hospital, your urologist could decide to take X-rays to check for any remaining stone fragments. Your urologist might wish to remove them if there are any. In roughly one to two weeks, you can resume your regular activities.