Orchidopexy: Treatment of Undescended Testicles
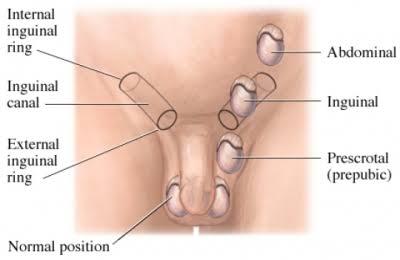
When one or both testes are absent from the scrotum, the testicle is considered undescended. The frequency is 3-4% of newborn boys and is particularly prevalent in preterm newborns. The majority of undescended testes occur on a single side (80%). In a lower proportion of instances (20%), they appear on both sides.
How Undescended Testicles Are Diagnosed
Many male babies and toddlers referred for assessment of an undescended testicle really have a retractile testicle. This is a testicle that usually lives in the low inguinal canal or high scrotum, but it may travel into the scrotum when the kid is sleeping, at rest, or in a warm bath. Retractile testes are often bilateral (found on both sides), and both sides of the scrotum are fully formed. A retractile testicle is one that can be maneuvered into the scrotum, totally released, and re-grasped without further manipulation. In this instance, as the youngster ages and the testicle grows, gravity will ultimately draw it into the scrotum.
If, however, the kid is six months old and the testicle must be repeatedly manipulated to move it into the scrotum, and it does not stay there after the examiner releases it, it is undescended and requires surgical repair. The five main reasons for surgically correcting an undescended testicle are:
Improve your odds of fathering a child, reduce the risk of damage to the undescended testicle, and correct any associated inguinal hernia.
To restore a normal scrotum look with two testicles instead of one, there is a danger of testicular cancer (see to “Surgical correction” below for information).
Male fertility (the capacity to father offspring) in the presence of an untreated one-sided undescended testicle varies from 40 to 65 percent. In contrast, fertility in a one-sided undescended testicle corrected before the age of six is around 80-90%. (The reduced reproductive rate associated with all undescended testicles is related to the higher temperature environment of the non-scrotal testis.)
A testicle in the inguinal canal (groin) is susceptible to crush damage because it is generally immobile and rests on top of tight ligaments and bone. Approximately 90% of inguinal testicles include a hernia-like sac, which predisposes to hernia development. The hernia will be corrected during the orchidopexy procedure.
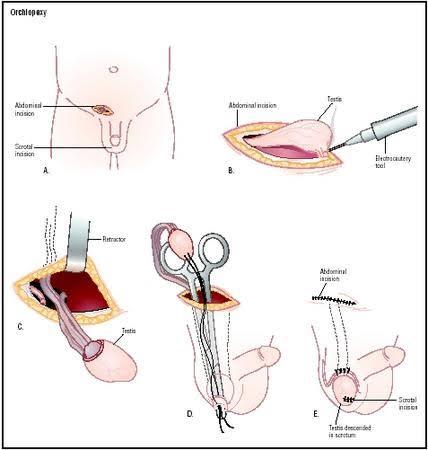
Surgical correction (orchidopexy).
Orchidopexy is a surgical treatment that involves inserting an undescended testicle into the scrotum. The procedure is done to lessen the danger of crush damage, rectify the hernia, and/or ameliorate the psychological effects of just having one testicle visible in the scrotum.
An orchidopexy does not, however, protect against the 8-10 times higher risk of testicular cancer in men with a history of undescended testicle. Furthermore, the timing of orchidopexy seems to have a little impact on the risk of testicular cancer in these individuals. Orchidopexy does, however, provide an important benefit: by shifting the testicle into the scrotum, surgeons may more easily monitor for symptoms of cancer in the future. Easier monitoring offers a higher likelihood of early diagnosis if a tumor develops.
Details of the Operation
A groin incision is used to conduct orchidopexy on a palpable undescended testicle. The aberrant attachments of the testicle in the inguinal canal are dissected, and the hernia sac (if present) is carefully separated from the testicular blood vessels and vas deferens.
The testicular artery’s length limits the capacity to bring the testicle into the scrotum. When the artery is exceptionally short, the testicle, blood supply, and vas deferens may be placed under the epigastric arteries and straight into the scrotum.
A testicle that is not located in the groin or scrotum might be in the abdominal cavity. These testicles (known as “nonpalpable” because they cannot be felt with the touch and “intraabdominal” because they are positioned in the belly) may occasionally be found with an ultrasound or CT scan of the abdomen. However, in other cases, testicular tissue is present but cannot be detected by any of these tests.
The only way to be confident that a testicle is totally missing is to directly see blind-ending testicular veins and a blind-ending vas deferens. The initial step in treating a unilateral nonpalpable testis (a testicle that cannot be identified by physical examination) is laparoscopy.
If laparoscopy indicates that the testicle is missing (i.e., the testicular veins and vas deferens meet at a dead end), no further treatment is required.
If the testicle exists but is atrophic (wasting away), it should be removed.
If the testicle is healthy, it may be moved via orchidopexy.
If the testicle is located near the groin, a normal orchidopexy may be done.
If the testicle is elevated (near the kidney), the testicular arteries should be trimmed and split in preparation for a second-stage orchidopexy in 3-4 months. During that time, the testicle will acquire a new blood supply via collaterals along the vas deferens, allowing it to be safely transported down into the scrotum.