What is Benign Prostatic Hyperplasia (BPH)?
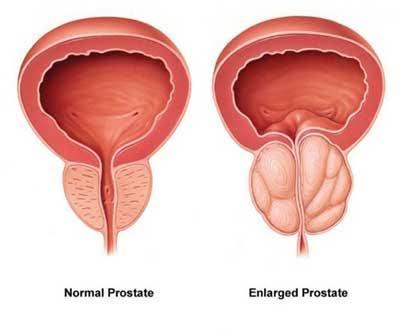
Benign prostatic hyperplasia (BPH) refers to the enlargement of the prostate and adjacent tissue. The prostate undergoes two primary phases of growth as a man ages. The initial phase occurs early in puberty, during which the prostate undergoes a twofold increase in size. The second phase commences at approximately age 25 and persists throughout the majority of a man’s life. With advancing age, the prostate may undergo enlargement. Benign Prostatic Hyperplasia (BPH) occurs when the prostate enlarges sufficiently to induce complications.
As the prostate hypertrophies, it exerts pressure on the urethra. The bladder wall thickens. With the passage of time, the bladder may deteriorate and become incapable of complete evacuation. The urine thereafter resides in the bladder. These issues contribute to several lower urinary tract symptoms (LUTS) associated with benign prostatic hyperplasia (BPH).
Symptoms of Benign Prostatic Hyperplasia
An enlarged prostate can obstruct or irritate the bladder. Frequent urination is a prevalent sign of benign prostatic hyperplasia (BPH). This may involve the necessity to urinate as frequently as every one to two hours, primarily during the night. Additional symptoms of BPH are enumerated below.
· Incomplete bladder evacuation: the sensation of fullness despite urination.
· Frequency: the necessity to urinate frequently, approximately every one to two hours.
· Intermittency: the necessity to halt and resume multiple times during urination.
· Urgency: the intense sensation of needing to urinate immediately, as if one cannot postpone.
· Reduced stream: a diminished urine flow.
· Straining: difficulty initiating urination or the necessity to exert force to urinate.
· Nocturia: the necessity to awaken at night more than twice to urinate.
Diagnosis
Numerous assessments exist for benign prostatic hyperplasia (BPH). The subsequent assessments are employed to diagnose and monitor BPH.
· International Prostate Symptom Score (IPSS) – If you experience any urinary alterations or symptoms, your physician may discuss the BPH Symptom Score Index with you. The American Urological Association (AUA) created this assessment to evaluate urine symptoms. This is frequently the initial step in diagnosing BPH. The score might classify BPH as mild to severe. You and your healthcare practitioner may discuss your results and medical history. This is occasionally referred to as the International Prostate Symptom Score (IPSS).
· Digital Rectal Examination – A digital rectal examination (DRE) is typically the subsequent procedure. During a digital rectal examination, you assume a lateral position or bend forward. The physician inserts a gloved, lubricated digit into your rectum to palpate the posterior aspect of the prostate gland. The healthcare provider is assessing for enlargement, discomfort, lumps, or indurations. This 10-15 second assessment is a crucial method for identifying issues.
· Urine testing – These assessments evaluate the efficiency of urine excretion. This indicates to the physician whether the urethra is occluded or obstructed. There exist various categories:
o Urinalysis – Urinalysis examines your urine sample to detect critical elements such as blood, indicators of infection, glucose, protein, and other variables that may inform your urologist with the aetiology of your symptoms. Urinalysis is employed to detect bladder carcinoma. It is imperative to consult your physician immediately if you experience haematuria, dysuria, or urinary retention.
o Post-void residual volume (PVR) – Post-void residual volume (PVR) quantifies the urine remaining in the bladder following urination. This is performed to identify the issue. It may also be performed prior to surgery.
o Uroflowmetry – Uroflowmetry quantifies the velocity of urine excretion. This is performed to identify the issue. It may also be conducted prior to surgery.
o Urodynamic study – A urodynamic pressure flow study assesses bladder pressure during micturition.
· Scans – These examinations are conducted to assess the dimensions and morphology of the prostate. Certain BPH scans comprise:
o Ultrasounds examine the internal structure of the body to assess the size and morphology of the prostate.
o Cystoscopy – is a procedure utilised to examine the urethra or bladder using a scope.
o Magnetic resonance imaging (MRI) and computed tomography (CT) provide more comprehensive scans. Surgery is performed if it is essential to restore the flow of urine. These scans offer a highly detailed representation of the prostate and its adjacent regions. It precisely illustrates the location and extent of prostate enlargement.
· Haematological Tests
o PSA – Blood tests for prostate-specific antigen (PSA) are utilised to screen for prostate cancer. The PSA blood test measures the concentration of PSA, a protein exclusively produced by the prostate gland. This blood test can be conducted in a laboratory, hospital, or healthcare provider’s office. Refrain from engaging in sexual activity for several days before the test, since this may artificially elevate the PSA levels. In a healthy prostate, minimal levels of PSA are detected in the bloodstream. An abrupt increase in PSA levels may indicate an underlying issue. A benign enlargement of the prostate can elevate PSA readings, as can prostate inflammation (prostatitis). The primary cause of an elevation in PSA levels is cancer.
Therapeutic Intervention
The primary therapies for BPH are:
1. Active Surveillance
2. Prescription Medications
3. Minimally Invasive Surgery
4. Simple prostatectomy
Active Surveillance
Frequently, BPH may necessitate solely active monitoring. Your BPH will be followed closely without active treatment, potentially through regular consultations with your urologist. An annual examination is prevalent. Your healthcare practitioner will assess for exacerbated or novel concerns prior to recommending any further actions. Diet and exercise are frequently advised for the prevention or management of symptoms. Active surveillance is optimal for males exhibiting mild to moderate symptoms. It is also a viable alternative for guys who are unconcerned by the effects of BPH.
Prescription Medications
Pharmaceuticals may potentially be a viable alternative for men with benign prostatic hyperplasia (BPH). Categories of pharmaceuticals encompass:
· Alpha blockers are medications utilised to alleviate the musculature of the prostate and bladder, hence mitigating symptoms of benign prostatic hyperplasia (BPH). They do not reduce the size of the prostate; nevertheless, they may enhance urine flow in the presence of a blockage. One advantage of alpha blockers is their immediate efficacy. Potential adverse effects may encompass dizziness, lightheadedness, weariness, and challenges with ejaculation. Men with moderate to severe benign prostatic hyperplasia (BPH) and those distressed by their symptoms are suitable candidates. Alpha blockers are not advisable if you want to undergo cataract surgery in the near future. Alpha-blocking medications encompass alfuzosin, doxazosin, silodosin, tamsulosin, and terazosin.
· 5-Alpha reductase inhibitors are medications that enhance urinary flow and reduce prostate size by inhibiting DHT. Dihydrotestosterone (DHT) is an androgen that can accumulate in the prostate, potentially leading to prostate enlargement. These medications may reduce the likelihood of BPH complications and the necessity for surgical intervention. Adverse consequences including erectile dysfunction and diminished libido. It is imperative to continue taking the medication to avert the recurrence of symptoms. These may be most suitable for individuals with significantly enlarged prostate glands. The prescription medications, dutasteride and finasteride, may require several months to achieve full efficacy.
· Combined therapy employs both an alpha blocker and a 5-alpha reductase inhibitor. Their combined efficacy may surpass that of any medicine administered individually in preventing the progression of BPH. Administering two medications may result in a greater incidence of side effects compared to the administration of a single medication. Potential adverse effects may encompass dizziness, erectile dysfunction, fatigue, and a decrease in blood pressure while transitioning from a seated or supine position to standing. A urologist may prescribe antimuscarinics for patients exhibiting signs of overactive bladder. Overactive bladder occurs when the bladder muscles contract involuntarily. It results in a recurrent and pressing necessity to urinate. It may result in incontinence (leakage). Antimuscarinics induce relaxation of the bladder musculature. Individuals with enlarged prostates are suitable candidates for this treatment.
Minimally invasive surgical procedure
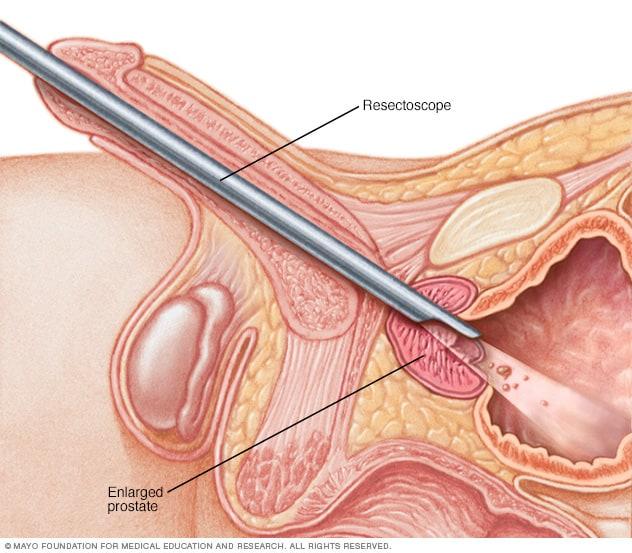
- Transurethral resection of the prostate (TURP) is a prevalent surgical procedure for benign prostatic hyperplasia (BPH). TURP use electric current or laser light to excise and eliminate tissue. This procedure is performed under anaesthesia using a resectoscope, which is introduced through the penis. The resectoscope delivers illumination, irrigation fluid, and an electrical loop. The loop incises tissue and occludes blood arteries. The excised tissue is expelled into the bladder and subsequently eliminated from the body via a catheter. Men with moderate to severe BPH symptoms who necessitate surgery may be suitable candidates for TURP. There exist two varieties of TURP.
o Monopolar Transurethral Resection of the Prostate (TURP)
o Bipolar Transurethral Resection of the Prostate
- Transurethral incision of the prostate (TUIP) is employed to enlarge the urethra when the prostate gland is diminutive but creates significant obstruction. In TUIP, the surgeon performs minor incisions at the bladder neck, where the urethra connects to the bladder, as well as in the prostate. This dilates the urethra and alleviates the pressure exerted by the prostate on the urethra, facilitating urination. The duration of the hospital stay ranges from one to three days. A catheter remains in your bladder for one to three days post-surgery. Certain males require subsequent therapy. Men who require surgery but choose to avoid a total prostatectomy are suitable candidates.
- Laser prostatectomy –
o Holmium laser enucleation of the prostate (HoLEP) – involves a surgeon inserting a resectoscope via the penis into the urethra. A laser utilised within the resectoscope eliminates surplus prostate tissue. No incisions are required, and there is minimal bleeding. A one-night hospital stay may enough. A catheter is employed, however it is often extracted the next day. Men with enlarged prostates seeking to evade more intrusive surgical options may be suitable candidates for this treatment. Men at an elevated risk of haemorrhage, such as those on anticoagulant therapy, may also be suitable candidates for HoLEP.
o Thulium Laser Enucleation of the Prostate (ThuLEP) – Thulium laser enucleation of the prostate (ThuLEP) resembles HoLEP but employs a distinct laser type. Similar to HoLEP, the surgeon inserts a resectoscope via the penis into the urethra. A laser utilised within the resectoscope eliminates surplus prostate tissue. Men with enlarged prostates seeking to evade more invasive surgical procedures may be suitable candidates for this treatment. No incisions are required, and there is minimal bleeding. A one-night hospital stay may enough. A catheter is employed, however it is often extracted the next day. Men at an elevated risk of haemorrhage, particularly those on anticoagulant therapy, may also be suitable candidates for ThuLEP.
- Simple prostatectomy entails the complete excision of the prostate gland utilising laparoscopic or robotic-assisted surgical techniques. The surgeon must possess proficiency in this procedure. This is exclusively available to males with the most substantial prostate glands. This constitutes a long-term remedy. You will likely remain in the hospital for many days post-surgery, and your activities will be restricted for a number of weeks. A catheter is typically required for one to two weeks during the healing process.
Anticipations Post-Surgery
In the majority of men, symptoms of benign prostatic hyperplasia (BPH) ameliorate following treatment. Post-surgery, the restoration of sexual function may require time. The majority of experts assert that if one could achieve an erection prior to surgery, the ability to do so post-operation is likely retained. Your orgasm is not anticipated to alter. In certain instances, males may encounter a condition in which semen enters the bladder instead of exiting through the penis (retrograde ejaculation). Infection, haemorrhage, and incontinence may also arise following certain BPH therapies. Scar tissue may develop in certain instances. Adverse consequences differ according on the selected treatment, and the majority of these effects are transient. Certain men require additional or alternative therapy for their BPH symptoms following initial treatment. It is imperative to inform your physician of any negative effects you may experience in order to receive assistance.