Pelviureteric Junction Obstruction
What is it?
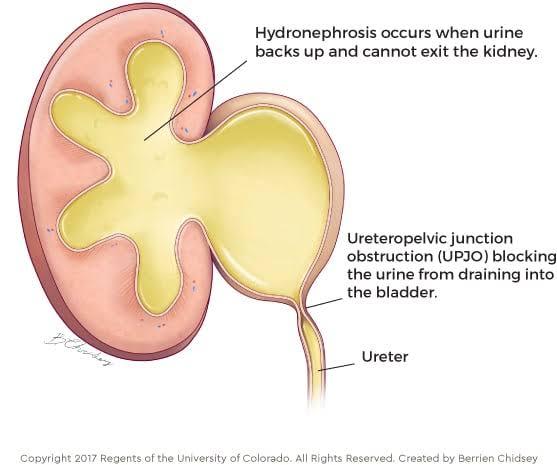
Pelviureteric junction obstruction (PUJO) refers to an impairment of urine flow at the junction of the pelvis (collecting system of the kidney) with the ureter (tube which takes urine to the bladder). What causes it? Often there is a short section of ureter, which is narrowed (see below). Sometimes there are additional blood vessels, which cross the ureter and may contribute to a blockage.
How does it present?
When there is restriction to urine flow, the urine builds up behind the blockage, distending the collecting system within the kidney. This can be seen on ultrasound, even before birth. After birth, PUJO may present with: – flank pain, often severe – urinary tract infection – abdominal mass – haematuria (blood in the urine) – incidentally (when ultrasound is performed for another reason)
What tests are performed?
Ultrasound
An ultrasound is usually the first indication of concern, particularly in babies or young children where no symptoms may be present. The ultrasound shows a number of important signs: – how severe the distension (stretching) of the collecting system is – what the parenchyma (kidney tissue) looks like – what the drainage tube (ureter looks like): usually not seen in PUJO – presence and state of the other kidney – what the bladder looks like
Nuclear medicine (MAG3, DTPA) – Specialised nuclear medicine studies can determine the function of each of the two kidneys relative to one another. They can give information regarding rate of drainage from each system. These should be performed in a paediatric centre to obtain the most reliable results. A small amount of radioactive material is injected through a needle into the child’s bloodstream and a special camera takes pictures of the kidneys and records the material passing through and draining from the kidneys.
What are the treatment options?
Many apparent PUJO cases are now identified on antenatal ultrasound. Some of these cases will settle spontaneously and not require active treatment. For some, treatment can be postponed until the situation worsens. The medical team will take into consideration a combination of factors to determine whether intervention is indicated. Often, monitoring with serial ultrasounds while the baby grows is appropriate. In some cases, early intervention is required to protect or salvage kidney function. When treatment is required, it involves an operation is called a ‘pyeloplasty’. This involves removing the narrowed section of ureter where the blockage is, rejoining of the remaining ureter to the renal pelvis.
What are the outcomes?
The most important aim of treatment and follow up is the preservation of kidney function. Many children improve as they grow, with stable or less distension being seen with time. Even if the dilatation persists but does not worsen, this is a positive sign. The child’s urine flow is increasing with body size – stable dilatation indicates there is no significant ‘blockage’ requiring surgery. For the children who require operative correction of the blockage, the success at salvaging or protecting kidney function from deterioration is very good (around 98% successful).
What is the follow-up?
Ultrasounds comprise the majority of the follow up imaging. This study is non-invasive, does not hurt and does not use any radiation. Sometimes, repeat nuclear scans are needed when the situation changes unexpectedly. The frequency of follow-up will depend on the severity of dilatation and the rate of any changes.
What is PUJO?
An impairment of urine flow at the point where the ureter (the tube that transports urine to the bladder) and pelvis (the kidney’s collecting system) meet is known as pelviureteric junction obstruction (PUJO).
Why does it happen?
The ureter frequently has a brief, narrowed segment (see below). A blockage may occasionally result from extra blood vessels that cross the ureter.
How does it present?
Urine accumulates behind the obstruction when urine flow is restricted, extending the kidney’s collecting system. Even before birth, this can be seen on ultrasound. Following birth, PUJO may manifest as:
· urinary tract infection – flank pain, frequently severe
· Abdominal mass
· Blood in the urine is known as haematuria
Which tests are conducted?
Ultrasonography
The first sign of concern is typically an ultrasound, especially in infants or young children who may not exhibit any symptoms. The ultrasound displays several significant indicators: The degree of distension (stretching) of the collecting system; the appearance of the kidney tissue (parenchyma); and the appearance of the drainage tube (ureter), which is typically absent in PUJO The appearance of the bladder; the existence and condition of the other kidney
Nuclear Scan
The function of each kidney in relation to the other can be ascertained through specialised nuclear medicine studies (MAG3, DTPA). They can provide details about each system’s drainage rate. For the most dependable results, these should be carried out in a paediatric facility. After injecting a tiny quantity of radioactive material into the child’s bloodstream via a needle, a specialised camera records the material’s passage through and out of the kidneys and takes images of them.
Which treatments are available?
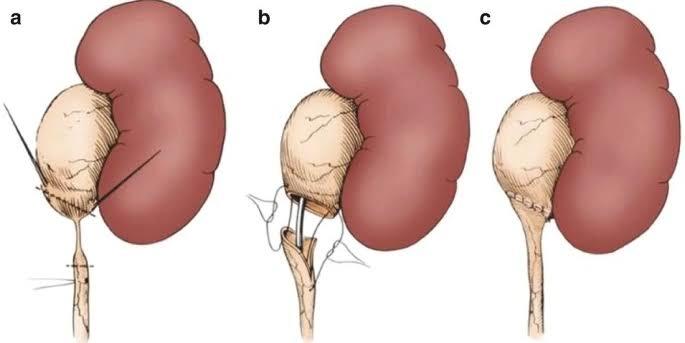
Prenatal ultrasound is now used to identify a large number of apparent PUJO cases. Some of these cases will resolve on their own without the need for active therapy. Some people may be able to put off treatment until things get worse. To decide whether intervention is necessary, the medical team will consider a number of factors. Serial ultrasound monitoring during the baby’s growth is frequently appropriate. Early intervention may be necessary in certain situations to preserve or restore kidney function. When therapy is necessary, a procedure known as a “pyeloplasty” is performed. This entails rejoining the remaining ureter to the renal pelvis after removing the constricted portion of the ureter where the obstruction is located.
What are the results?
Preserving kidney function is the primary goal of treatment and follow-up. As they get older, many kids get better; over time, they show stable or less distension. This is encouraging even if the dilatation continues without getting worse. The child’s urine flow increases as their body size does; stable dilatation suggests that there isn’t a serious “blockage” that needs to be surgically removed. It is very successful (about 98%) to save or prevent kidney function from deteriorating in children who need surgical correction of the blockage.
What’s the next step?
The majority of the follow-up imaging consists of ultrasounds. There is no radiation used in this non-invasive, painless study. Repeat nuclear scans may occasionally be required when circumstances suddenly change. The degree of dilatation and the rate of any changes will determine how frequently you need to follow up.