Urethral Stricture
A urethral stricture: what is it?
A urethral stricture is a narrowing brought on by scarring of the corpus spongiosum and urethral lining. Strictures that run the whole length of the urethra or less than 1 cm in length are both possible. Although they can appear anywhere along the urethra, the bulbar region is where they are most frequently observed.
Which factors lead to urethral strictures?
The stricture’s location determines the most likely cause. In general, the most frequent explanations are:
· Idiopathic and inflammatory conditions: lichen sclerosus (LS), also called balanitis xerotica obliterans (BXO), and sexually transmitted infections (STIs) like gonorrhoea are examples of urethral infections or inflammations that cause these conditions.
· Pelvic trauma linked to a fractured pelvic bone;
· Trauma caused by injury to the urethra, such as a fall against a bicycle crossbar;
· Iatrogenic caused by medical intervention, such as: urethral catheterisation; radiotherapy or surgery to nearby organs; recurrent urological procedures involving the passage of instruments along the urethra; or
· Congenital inherited conditions For instance: hypopadias (or as a consequence of prior surgery to address hypopadias)
What signs of a urethral stricture could I experience?
You might not experience any symptoms if your strictures are minor. You might encounter one or more of the following with more stringent strictures:
1. Urinary tract infections,
2. dribbling of urine after urination,
3. weak ejaculation force and low ejaculate volume,
4. poor urinary flow and the need to strain to pass urine,
5. spraying or splitting of the urinary stream, and
6. pain during urination are some of the symptoms.
How can a stricture be identified?
If your bladder does not empty completely on an ultrasound scan after you have passed urine or if your urinary flow rate is decreased, you may have a stricture. The following methods can be used to diagnose a stricture:
· examination, particularly if the narrowing is visible at the tip of the penis;
· failure to pass a telescope or catheter during the investigation of your urinary symptoms, particularly if the stricture is near the bladder;
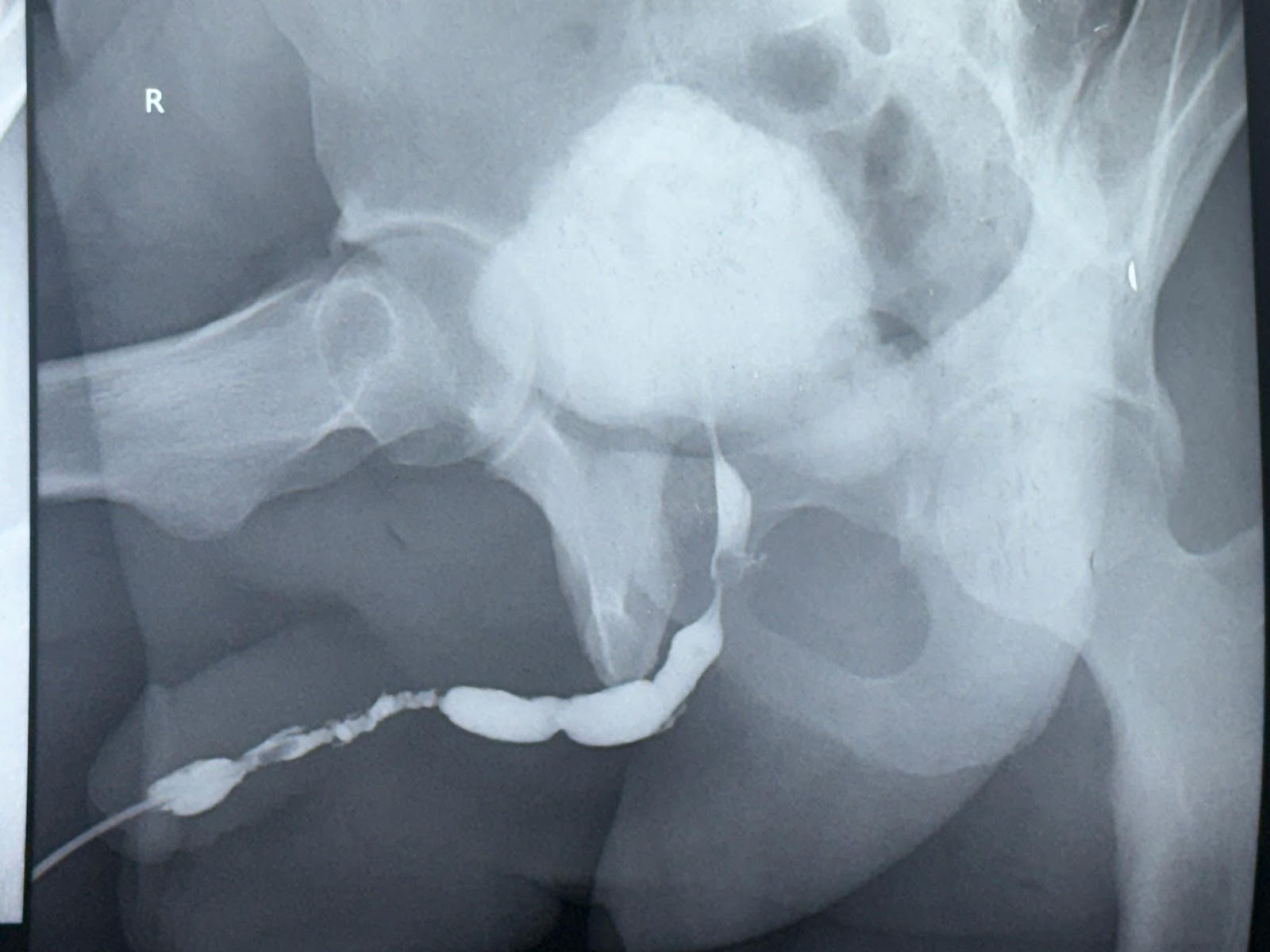
· urethrogram, which is an X-ray in which the anatomy is shown by the use of contrast medium (dye) inserted into your urethra;
· ultrasound; and
· MRI.
TREATMENT
Your preferences as the patient, the location and duration of your stricture, the reason behind it, any prior treatments you may have had for it, and your overall health all influence the kind of treatment we suggest.
DILATATION OF THE URETHRA – To enlarge the constricted space, we insert a metal or plastic dilator into your urethra while you are under anaesthesia. We might then instruct you on how to insert a comparable dilator or “slippery” catheter into your urethra.
INTERNAL URETHROTOMY (OPTICAL) – To cut the stricture, we insert a telescope through your urethra while you’re under anaesthesia. The scar tissue that is causing the narrowing is opened but not removed by this. For at least 24 hours following the procedure, you will typically require a bladder catheter, which is a tube that passes through your urethra and into your bladder. Usually, it is done on a case-by-case basis.
URETHROPLASTY – In order to prevent the stricture from returning, this intricate procedure entails repairing the damaged urethral segment. Compared to urethral dilatation or internal optical urethrotomy, it has a higher risk of adverse effects, requires a longer duration of anaesthesia, and is an open (cutting) procedure.
· ANASTOMOTIC BULBAR URETHROPLASTY – If your stricture is short, anastomotic bulbar urethroplasty involves cutting out the narrowed portion and reattaching the healthy ends.
· BUCCAL MUCOSAL GRAFT URETHROPLASTY – The buccal mucosa graft urethroplasty procedure involves cutting open the narrowed area of your stricture and using a piece of your cheek lining (buccal mucosa) as a graft to widen it. o enhanced For long, tight strictures, anastomotic buccal mucosa graft urethroplasty involves cutting out the diseased portion, joining the healthy ends, and using a buccal mucosal graft to enlarge the urethra.
· PERINEAL URETHROPLASTY – urethrostomy of the perineum. In this procedure, the diseased urethra is brought out to the skin surface in the perineum (between the anus and the back of the scrotum, as shown in the picture) in order to “short-circuit” it. Only when the bulbar urethra is healthy and has a normal diameter is it used.
SUPRAPUBIC OR LONG-TERM URETHRAL CATHETERISATION – We might advise implanting a long-term catheter if you have several health issues or if you would prefer not to undergo invasive treatment.