Vesicoureteral Reflux
Vesicoureteral reflux (VUR): what is it?
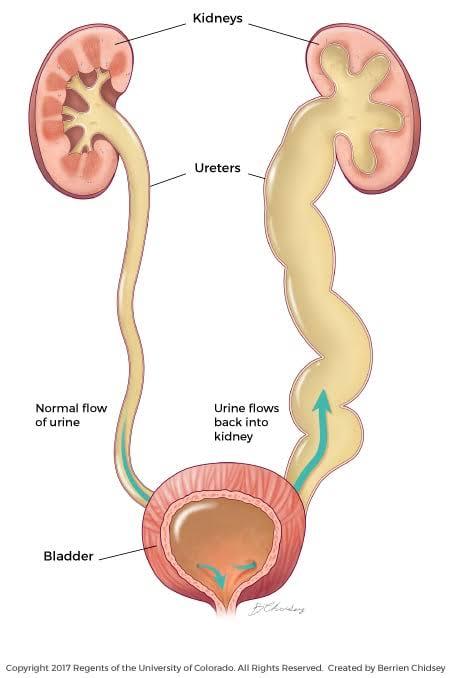
A disorder known as vesicoureteral reflux (VUR) occurs when urine runs in the incorrect direction. Your urine runs backward from your bladder rather than down into your ureters and bladder, where it remains until you urinate.
The urine usually flows down your urinary system, which is a one-way valve. Once urine reaches your bladder, this valve-like mechanism stops it from returning up into your ureters. Pee should normally flow like this: The kidneys generate urine. You normally have two kidneys. Urine is transported from your kidneys to your bladder by two slender, muscular tubes called ureters. Your urine is stored in your bladder. It is capable of balloon-like expansion. Your urethra is where your urine exits your body. Your urine exits through a hole called your urethra. When you have VUR, urine refluxes, or flows back, from your bladder into one or both ureters and, occasionally, to one or both kidneys. The most common cause of it is a problem that keeps the one-way valve from operating properly.
Vesicoureteral reflux disease (VUR) primarily affects newborns, infants, and young children under the age of two, while it can also occur in older children and, in rare cases, adults.
If your child’s urine flows in the wrong direction, bacteria may enter their kidneys and create an infection. If kidney infections are not treated, they might result in irreversible kidney damage.
The severity of your child’s symptoms, their age, and other variables all affect how they are treated with VUR. Treatment may not be necessary for mild instances, and some kids outgrow VUR. However, some kids require medicine or surgery to treat VUR in order to prevent kidney damage.
Types of VUR
Unilateral reflux is a type of VUR that only affects one kidney and ureter. Bilateral reflux is a type of VUR that impacts both the kidneys and the ureters.
VUR comes in two varieties: main and secondary.
Primary VUR: The majority of VUR cases are primary, typically affecting only one kidney and one ureter (unilateral reflux). Your child has a primary VUR if their ureter isn’t connected to their bladder correctly from birth. Pee refluxes from the bladder to the ureter and, in certain situations, the kidney because the flap valve that separates the ureter from the bladder wall doesn’t seal properly.
Secondary VUR: Secondary VUR happens when a blockage in the urinary tract raises the pressure and forces urine back up into your child’s kidneys, ureters, or bladder from the urethra. An irregular tissue fold in the urethra also known as POSTERIOR URETHRAL VALVE may be the cause of the obstruction, which prevents urine from easily exiting your child’s bladder. A nerve issue that prevents the bladder from being stimulated to discharge urine could be another cause of secondary VUR. Bilateral reflux, which affects both ureters or both kidneys, is common in children with secondary VUR.
What are the stages of vesicoureteral reflux (VUR) ?
There are five grades that make up the VUR phases. One is the mildest kind of VUR, while five is the most severe. The degree to which urine backs up into the urinary tract is the basis for the grading system.

The breakdown of grades is:
Grade 1: The ureter is a normal width, but the urine travels backward up into it.
Grade 2: Pee backs up into the renal pelvis, which is where the kidney and ureter connect, and a ureter. The ureter and renal pelvis have not widened.
Grade 3: Due to pee backing up, the ureter(s), renal pelvis, and calyces—where urine collecting starts in the bladder—are mildly to moderately enlarged.
Grade 4: Due to excessive pee backing up, the kidney pelvis and calyces are also substantially enlarged, and the ureter or ureters are curved.
Grade 5: There is significant enlargement and distortion of the ureter or ureters. Due to an excessive volume of urine backing up, the renal pelvis and calyces are quite big.
What is the prevalence of vesicoureteral reflux?
Children with vesicoureteral reflux (VUR) range from 1% to 3%. Females make up about 75% of children with VUR.
Causes and Symptoms
What signs of vesicoureteral reflux disease (VUR) are present?
A youngster with vesicoureteral reflux (VUR) frequently exhibits no symptoms. Urinary tract infections (UTIs) are the most common when symptoms are present. According to some estimates, VUR affects 30% to 50% of kids who have a UTI.
A child’s UTI symptoms include:
- having to urinate more frequently.
- ache or burning during urinating.
- discomfort in their lower back or abdomen (flank pain).
- Just a few drops of urine at a time.
- cloudy or foul-smelling urine.
It can be more challenging to identify UTI symptoms in infants. They can get fussy or lose their usual appetite.
What complications might vesicoureteral reflux (VUR) cause?
Vesicoureteral reflux disease (VUR) in children can lead to the following complications:
- bladder and kidney infections are examples of urinary tract infections (UTIs).
- bladder issues, such as bedwetting, urine retention, and incontinence.
- elevated blood pressure.
- Nephrotic syndrome,
- kidney damage,
- kidney scarring, and infrequently,
- chronic kidney failure.
The majority of kids with VUR heal without any lasting issues.
Testing and Diagnosis
How is the diagnosis of vesicoureteral reflux disease (VUR) made?
Physicians that specialize on kidney and urinary tract disorders are known as pediatric nephrologists and pediatric urologists. For your child’s care, your pediatrician is probably going to recommend one or both of these specialists.
To identify vesicoureteral reflux (VUR), they could prescribe the following tests:
VCUG, or voiding cystourethrogram: A VCUG is a pre-, during-, and post-urination X-ray imaging of the bladder and urethra. Your child’s bladder is filled with a specific dye that may be seen on an X-ray by inserting a tiny catheter into the urethra. Urine moving backward from the bladder into the ureters is visible on the X-rays. This procedure is carried done by a clinician in a hospital, outpatient facility, or their office. Sedation may benefit certain kids, but anesthesia is not required.
Ultrasound: Using sound waves, this painless and safe imaging method produces pictures of your child’s whole urinary tract, including their kidneys and bladder. The study takes place at a hospital, outpatient clinic, or doctor’s office. If you or your healthcare provider wish to prevent exposure to radioactive material or X-ray radiation, a provider may do an ultrasound prior to a VCUG or RNC. A person can find out if their unborn child has VUR during pregnancy if a fetal ultrasound reveals symptoms of the condition, such as enlarged kidneys.
A scan of dimercaptosuccinic acid (DMSA): This imaging test determines whether kidney UTIs caused scarring to form in your child’s kidney.
A nuclear scan known as a radionuclide cystogram (RNC) entails injecting radioactive material into your child’s bladder. The radioactive substance is then detected by a scanner when your child is urinating or after their bladder has been emptied. A radiologist interprets the images after a properly trained technician performs the operation in a hospital, outpatient facility, or healthcare provider’s office. Although your child won’t require anesthetic, some kids might benefit from sedation. Though it doesn’t give as much information about the structure of the bladder, RNC is more sensitive than VCUG.
Management and treatment
How does one treat vesicoureteral reflux disease (VUR)?
The assistance of a healthcare professional is necessary for managing VUR. The age, symptoms, kind, and severity of your child’s VUR will determine the available treatment options. Among the treatments are surgery, short-term catheterization, injectable dissolvable bulking agents, antibiotics, and other drugs. Together with your doctor and other experts, you will go over these treatment choices and decide which is best for your child’s VUR.
Treatment of primary VUR
As people age, primary VUR may get better (usually by age 5). Waiting and seeing is sometimes the best course of action. In other cases, medicine or surgery are required.
Drugs
Primary VUR frequently gets better as your child ages and their urinary tract anatomy develops. To treat or prevent a urinary tract infection (UTI) in the meantime, your doctor will prescribe an antibiotic.
There is substantial debate surrounding the use of long-term antibiotics to prevent UTIs. Antibiotic resistance may result from prolonged usage of antibiotics. Preventive antibiotics are mostly advised by the American Academy of Pediatrics (AAP) for children with higher VUR grades (while waiting to see if they outgrow VUR).
Operation
For primary VUR, medical professionals employ a variety of surgical techniques. In order to stop urine from flowing backward, surgery aims to repair the one-way valve mechanism, which connects the bladder and ureters.
Reimplantation of the ureter
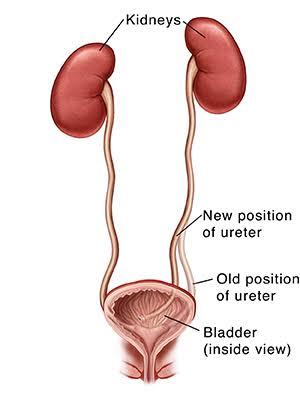
A ureteral reimplant is the gold standard surgical method for correcting VUR. In order to prevent urine from refluxing back up into the ureter, the reimplant aims to establish a flap-valve mechanism, which entails rerouting the ureter in the bladder wall with an appropriate length of tunnel. Your child’s surgeon may choose to undertake this procedure laparoscopically or openly, making an incision in your child’s abdomen. The advantages and disadvantages of each procedure, along with any potential adverse effects, can be discussed with you by your child’s surgeon. General anesthesia is necessary for surgery, and a brief hospital stay may be necessary.
Bulking agent that can be injected
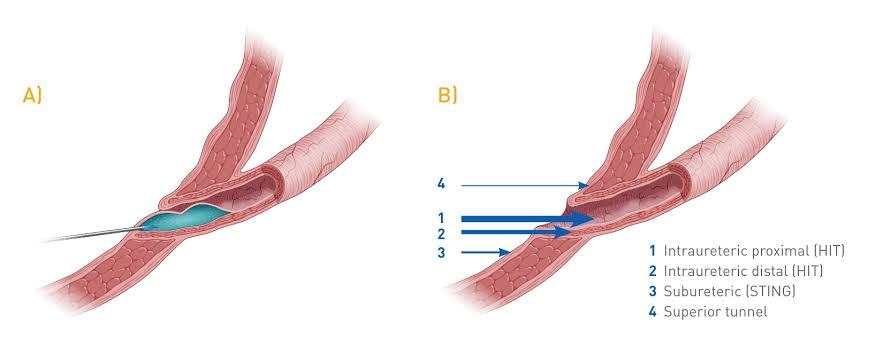
Using a gel-like liquid called hyaluronic acid/dextranome (Deflux®) is another method for primary VUR. A tiny amount is injected by your child’s healthcare practitioner into the wall of their bladder, close to the ureter’s entrance. Urine flow backward is impeded by this injection, which causes a bulge in the tissue and functions as a valve. Even though it’s an outpatient procedure—your child leaves the hospital that same day—general anesthesia is still necessary. The dangers and advantages of this kind of treatment can be discussed with you by your child’s healthcare professional.
Treatment for secondary vesicoureteral reflux (VUR)
Secondary vesicoureteral reflux (VUR) is treated by medical professionals either clearing the obstruction or enhancing the bladder’s ability to empty. Surgery to clear a blockage or fix an atypically formed bladder or ureter are possible forms of treatment.
Antibiotics for the treatment or prevention of UTIs
Intermittent catheterization involves passing a tiny tube through the urethra to the bladder in order to drain it.